 The current standard of practice is to change a short peripheral catheter when it is clinically indicated. This means that the presence of any sign or symptom of a complication indicates the need for catheter removal. We are no longer changing or rotating peripheral catheters based on the clock (72 to 96 hours) or a calendar (3 or 4 days). Many well-designed randomized clinical trials have demonstrated that the outcomes are equal for those that are changed at a specific time interval versus those changed when clinically indicated. This new standard brings up many questions for changes in clinical practice including
It is important to remember that this practice change is really only occurring in the adult patients. This has been the standard of practice for pediatric patients for many, many years as a set time interval for changing a peripheral catheter on an infant or child has never been applied. In 2012, INS released a position paper on the frequency of assessing peripheral catheter sites. The paper provides detailed guidance on the frequency of assessment based on the type of fluids and medications being given and many patient factors such as age and ability to communicate with the nursing staff. The frequency of assessment ranges from every 5 minutes for a vesicant medication to every 4 hours for a nonvesicant infusion in an awake and oriented adult. This assessment should include visual assessment, palpation, and obtaining comments from the patient about how it feels. This assessment should include all signs and symptoms of infiltration/extravasation, phlebitis, thrombosis, infection, and nerve injury. To review this position paper and several others from the Infusion Nurses Society, click here. The dressing on a peripheral catheter should be changed if it is wet, dirty or non-adherent to the skin. Otherwise, it should remain intact for the entire catheter dwell time. I am not aware of any healthcare facilities that have greatly altered the wording of their assessment policy for peripheral catheters. Primary care nurses may only look at the site and ask the patient how it feels but this may allow for many complications being missed. The only documentation may be a check mark on a specific form or nothing at all if charting by exception is the routine practice for documentation. Where I see problems is when I review medical records for malpractice lawsuits. In most of these cases, the catheter was used for an injection or infusion without a complete assessment. With a thorough assessment the nurse should have recognized early signs or symptoms of complications and that the catheter should not be used for infusion. Simply looking at the site will not allow the nurse to detect changes in skin temperature or induration. Often, gentle palpation will elicit tenderness that the patient may not have previously recognized. Prior to giving any drug, the INS Standards of Practice call for aspirating for a blood return. Many would argue that this is not a reliable test, but it cannot be disregarded in the complete assessment process, especially when giving a vesicant medication. This would require that the nurse understand the nature of the drug being given. Vesicants are not limited to oncology drugs. Promethazine, many vasopressors, all calcium preparations, contrast media agents, and some antibiotics are vesicants. To safely give a vesicant medication, the site must be free from all signs and symptoms of all complications, flush easily without any resistance, produce a blood return that is the color and consistency of whole blood, and allow for a free-flowing gravity infusion. It is also important to compare both extremities for changes in size. Infiltrations may not appear as a swollen area near the catheter tip. If compartment syndrome is happening, the entire forearm will appear larger than the opposite arm. None of these steps should be overlooked. One other problem is for the nurse to ignore a patient’s complains of some type of discomfort. The nurse may tell the patient that this is “normal,” or “all patients complain about this drug.” Discomfort or pain of any kind at a peripheral catheter site is an indication of a complication and is adequate reason to change that catheter. So no complaint should be ignored! Routine assessments that reveal no problems may not require documentation, especially if using charting by exception. However, without documentation how can the nurse prove that it was actually done? Prior to giving any vesicant medication, the complete site assessment including the presence or absence of a blood return should be documented. Nursing actions that are not documented have no proof that this assessment was done. Even an I.V. infusion of 5% dextrose in 0.45% sodium chloride can produce nerve damage when enough fluid has been pumped into the subcutaneous tissue. At a minimum, I would recommend
We offer a free poster which includes all the components of a catheter assessment. Download it from our website by clicking here.  We are pleased to announce that the new online continuing education course is now ready. This course took a year to create and is a strong source for your evidence-based practice. We have analyzed more than 100 studies to bring you the results. Questions that are answered in the course include:
These and many other questions are addressed in this course. After completion of this course, the learner will be able to:
The course awards 5 contact hours after successful completion. In honor of I.V. Nurses Day on January 25, we will offer a discount for this course. The regular registration fee is $149. For a limited time, the fee is $119. Register today and learn the most recent evidence-based practices for blood sampling.  Checking for a blood return is a significant component of a complete catheter patency assessment. Two standards of practice from the Infusion Nurses Society address this important step – Standard 61, Parenteral Medication and Solution Administration and Standard 45 Flushing and Locking. These statements do not limit the need to check for a blood return to a certain type of catheter or medication, making it important to obtain a blood return from both peripheral and central catheters prior to giving all medications. The reason for these standards is to prevent unnecessary complications such as infiltration or extravasation. The blood return should look like whole blood with the same color and consistency, however there are no requirements that you be able to aspirate a specific amount of blood before using the catheter. Many times, it seems impossible to obtain a blood return, leaving you to think that the catheter may not be functioning properly. Frequently the technique used for aspiration is the cause of the problem. Here are a few technique tips to ensure a blood return.
Failure of these step to produce a blood return means that the catheter is not functioning properly. Other steps in assessment include looking at the site to check for color changes (redness or blanching), fluid leakage from the puncture site, or swelling. Sometimes you will have to compare both extremities to see that swelling is present with a peripheral catheter. This is because fluid is accumulating in compartments of the arm and it is not appearing as a raised swollen area at the catheter tip. Flush the catheter with normal saline to check for resistance. Palpate the site before and during the flush. Did the patient complain of any discomfort when palpated? Did you feel any temperature change at the site? Did you feel the flush solution moving through the vein or feel fluid accumulating at the catheter tip? Finally, listen to everything the patient tells you about how the entire area feels. Flushing a central venous catheter whose tip has migrated to the jugular vein will cause the patient to hear a gurgling sound or running stream. Complaints of pain or discomfort in strange locations of the chest, neck, or upper abdomen could be related to the catheter. Before any medication is given through the catheter, you need to ensure that the site is free from all signs and symptoms of complications, that the patient has no complaints about the site, and that a blood return can be easily obtained. Many may think that a blood return will not provide useful information from a short peripheral catheter, but it is an important part of your assessment. A peripheral vein may have an additional puncture that allows fluid to leak into the tissue but you still get a blood return. That is why it is important to perform a complete assessment looking for all signs and symptoms. To download a poster that might be useful in teaching other nurses about this process, go to our website – hadawayassociates.com and scroll down to the Free Poster download. 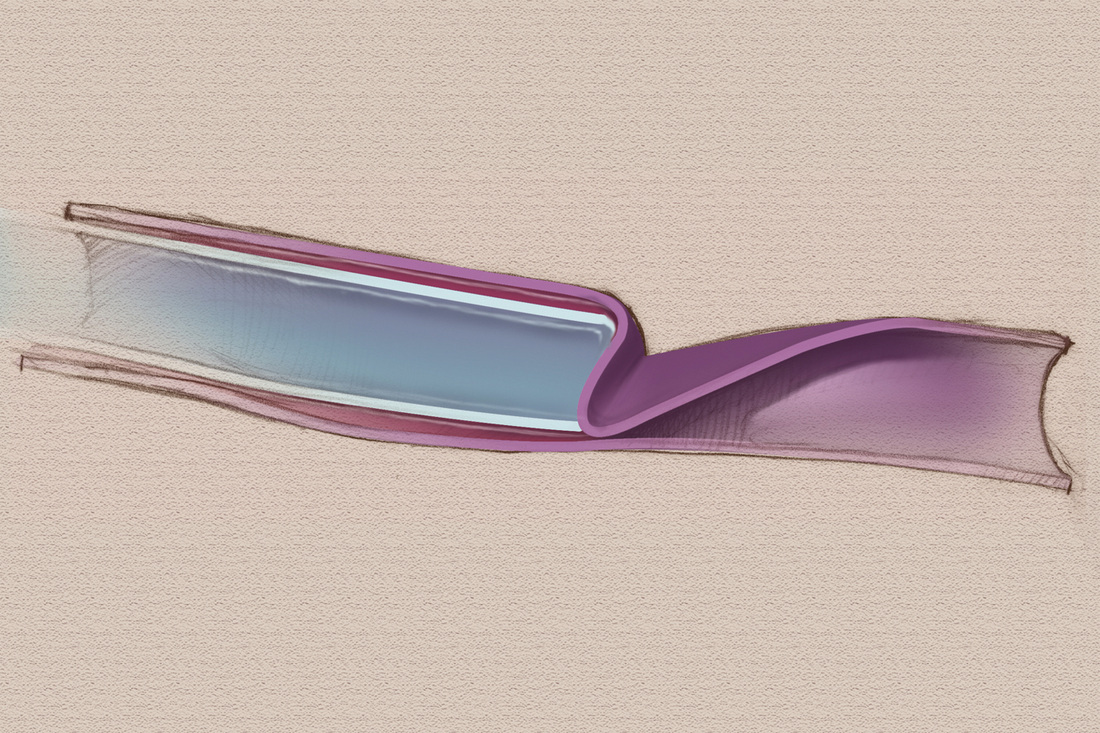 Collapsed peripheral vein wall occluding blood return 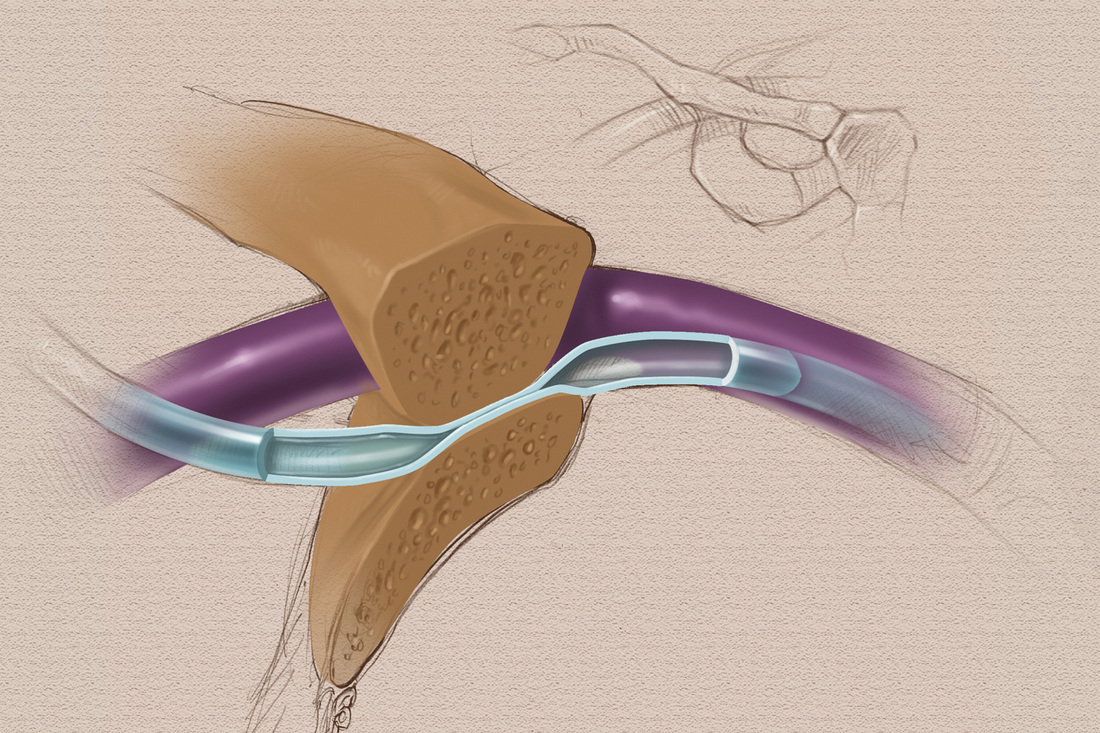 Subclavian vein insertion with catheter pinched between clavicle and first rib |
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861