|
Shortages of I.V. normal saline in liter bags continue with no end in sight. Manufacturers are still using allocation processes to determine which facility receives a designated amount of saline solution, typically an amount less than what would normally be ordered. The problem is also affecting compounding pharmacies in all communities and their ability to provide IV medications for alternative settings.
The majority of the problem is falling to pharmacists to chase whatever saline solutions might be available on a daily basis. Additionally prescribers have been asked to alter the solutions being given to patients. For example, 0.45 % sodium chloride or 5% dextrose/0.45% sodium chloride could be substituted for 0.9% sodium chloride. The FDA anticipates that the shortage will end in early 2015 but many experts have their doubts. To read a recent report, click here . What do these shortages mean for your practice? Has it changed the way you deliver IV medications? My concern is the use of bags of normal saline as the carrier fluid for piggybacking IV medications. Most hospitals now require infusion pumps for delivery of all fluids including piggybacked medications. The Infusion Nursing Standards of Practice recommends backpriming so that the secondary piggyback set can remain connected to the primary continuous infusion set. This practice reduces manipulation of the IV sets and reduces the contamination and risk for CLABSI. Normal saline is used as the “carrier” fluid if the primary continuous fluid has medication added to it that could be incompatible with the secondary medication. When the continuous fluid is no longer required and the intermittent medication is to continue, the infusion pump is still used to regulate the medication flow rate. This leaves a significant amount of medication in the infusion pump set that needs to reach the patient, so again saline is required. Has your hospital found a way to eliminate the need for this saline as a carrier fluid? Does your facility still require the infusion of I.V. medications be controlled by an infusion pump? Infusion by gravity would mean that much less fluid is left in the IV set and eliminate the need for the saline to flush the IV set – this was common practice about 15 to 20 years ago. But gravity infusion means an increase in nursing time to count drops and regulate infusion rates – a practice that many nurses have never learned. What other infusion practices have changed due to the saline shortages? We encourage you to share your ideas about dealing with this saline shortage.
37 Comments
 Yes, their goal is data on One Million Peripheral IV catheters (aka, OMG-PIV)! For sure this is an aggressive goal, but one well worth the effort.
Currently the Alliance for Vascular Access Teaching and Research Group (AVATAR) at the Griffith University in Australia has about 100 hospitals across the USA and nearly 500 hospitals from 50 countries participating. Participation by other hospitals is definitely wanted. AVATAR is the group of researchers who performed the studies that drove changes in the standards of practice from routine site rotation of peripheral catheters at 72 to 96 hours to removal when clinically indicated. Briefly this is a low risk audit on peripheral catheters with no intervention. The reason behind the study is that over a billion short peripheral catheters are inserted every year across the globe yet we have next to no data on how they are managed. About 40% of patients will have at least one catheter fail during their hospitalization either from accidental dislodgement, infiltration, phlebitis, or occlusion. That is a huge number of unnecessary venipunctures, catheters, nursing time and other resources. Here are a few more points about the study:
To learn more about this valuable study, go to their website at http://www.omgpivc.org If your hospital is interested in participating in this study, please contact Evan Alexandrou RN MPH| Lecturer Email: E.Alexandrou@uws.edu.au School of Nursing and Midwifery | University of Western Sydney Advanced Practice Nurse |Central Venous Access & Intensive Care|Liverpool Hospital Adjunct Senior Research Fellow| Griffith Health Institute Center for Health Practice Innovation| Alliance for Vascular Access Teaching and Research Group | Griffith University Conjoint Lecturer|South West Sydney Clinical School|Faculty of Medicine |University of New South Wales 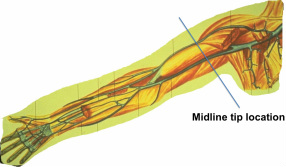 A few months ago, a new study was published about infusion of Vancomycin through one of the new types of midline catheters. The study challenged the Infusion Nursing Standards of Practice restrictions for pH of 5 to 9 through a midline catheter. Click here to read the abstract of the study http://www.ncbi.nlm.nih.gov/pubmed/24811603
An abstract of an editorial about this study can also be read by clicking here. http://www.ncbi.nlm.nih.gov/pubmed/24811587 On several online discussion groups and at the recent AVA conference, there were presentations, much discussion and lots of confusion! Many are now asking if it is time to change policy about use of a midline catheter. We will continue this discussion (and hopefully clear some of the confusion) on a videoconference planned for Thursday, October 16 from 1 pm to 2:30 pm. If registration exceeds our capacity, the presentation will be repeated at 3 pm to 4:30 pm. Learn more details and the process for registration here. Register early because computer connections are limited. Our new pricing structure allows for any size group to attend this presentation using the same (one) computer connection, however this method does not allow for awarding continuing education. We are eager to continue this discussion and hear your thoughts and questions.  Is this a new phrase for you? It was for me, but once I read the information it makes perfect sense along with supporting what nurses frequently see in clinical practice.
A recent group of experts met to create a literature review and consensus document about skin injury associated with medical adhesives. This report provides a great explanation of the various types of medical adhesives available and how they work. Identification and explanation of different types of skin injury (with pictures) are included, along with a brief description of pathophysiology and epidemiology. Although it is easy to label all skin injury as an “allergy” to the adhesive, that is least frequent problem. Knowing the actual type of injury and causes can aid in changing the situation for your patients. The report also contains recommendations for the correct way to apply and remove all adhesive products. All vascular access devices require some form of engineered stabilization/securement device with the most common ones involving some type of adhesive, but at the same time skin integrity is critical. Click here read the entire report. Don’t miss this great resource to assist with improving patient care. 
Today, the role of nurses in malpractice legal claims is changing. The following discussion is taken from the CNA Healthpro Nurse Claims Study: An Analysis of Claims with Risk Management Recommendations 1997-2007.
Nurse as Clinician While nurse-as-custodian claims continue to be asserted, plaintiff’s lawyers have now begun to pursue claims that focus on the nurse as a clinician, responsible for using professional judgment in the course of treatment. In these claims, nurses are perceived as highly skilled and educated professionals who are charged with making clinical observations, exercising discretion and taking appropriate treatment actions based upon a patient’s changing clinical picture. This shift reflects, to some extent, the increasing number and importance of specialties and areas of expertise within the profession. The following are examples of the new paradigm of nursing claims:
This shift has afforded increasing opportunities for plaintiff’s attorneys to name nurses as defendants in medical malpractice lawsuits. Mistakes made by nurses in their role as “custodian” were infrequent, and such mistakes led to easily understood claims that could be resolved without resorting to litigation. However, the new generation of “clinician” claims permits nurses to be included in any case in which a patient receiving complex treatment has a poor outcome.” It is no secret that the number of nurses named in lawsuits is increasing. One other trend is for the nurse or nurses to be the only named defendants left in the case after the physician and employer has been excused from the case. This is increasing the demand for nurses to be able to act appropriately as clinicians. Examples include increasing numbers of cases involving catheter-related bloodstream infection and I.V. medication adverse events. We have seen a decrease in Infusion Teams in many hospitals, putting the responsibility for safe administration of all I.V. fluids and medications in the hands of the primary care nurse. These cases are also holding the nurse accountable for the outcomes of his/her actions. In addition to cases involving mechanical catheter problems that produced a local complication such as extravasation, there is an increase is cases involving monitoring for adverse reactions to I.V. medications such as ototoxicity, nephrotoxicity, red man syndrome, and cardiac arrhythmias. Protect yourself by knowing and performing the correct process for I.V. medication administration. But also know the possible adverse events that can happen with each I.V. medication and document all components of your assessment to identify and reduce those adverse events. Nurses are required to act as clinicians rather than simply caring out the tasks prescribed by the physician. This requires knowledge and critical thinking along with psychomotor skills of catheter insertion. Click on the link below to download the complete report on nurse claims. |
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861