Definitely Yes!
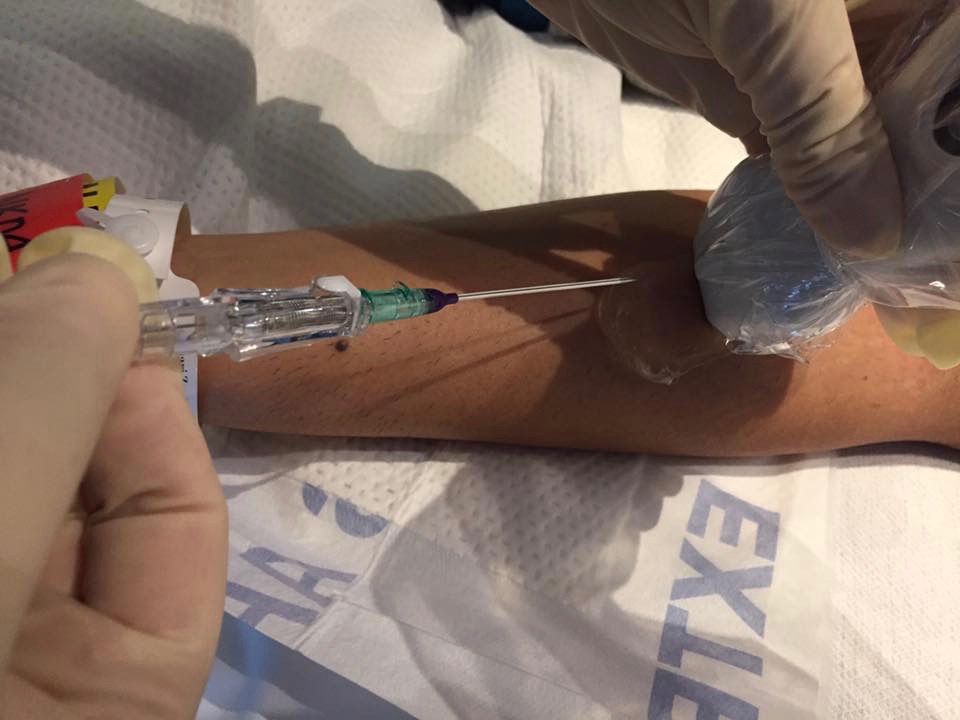
The 2016 Infusion Therapy Standards of Practice call for use of a large, sterile transparent membrane dressing over the probe for peripheral catheter insertion or a sterile probe cover along with sterile gel (page S45). Also, these standards support increased attention to strict aseptic technique by using sterile gloves when placing a peripheral IV catheter. (page S65). There are several objections to these standards with some citing the cost of sterile probe covers. Others cite the possible conflict with the Use of Ultrasound to Guide Vascular Access Procedures, from the American Institute of Ultrasound in Medicine (AIUM). This document can be found at http://www.aium.org/resources/guidelines/usgva.pdf This document states that maximum sterile barrier precautions are not needed for peripheral IV access, but goes on to state that a sterile probe cover or a transparent film dressing may be placed over the probe and that sterile gel is preferred. The INS Standards consider one aspect of care not addressed by the AIUM guidelines. The standard for removal of a PIVC is now based on clinical indications and not removal by a certain number of days or hours of dwell time. Many clinicians automatically assume that this means these catheters can be allowed to dwell for extended periods of time. Research shows that the actual dwell time for PIVC is far less than 72 to 96 hours, with most failing less than 48 hours of dwell. Longer dwell times are possible but we must use every tool for strict aseptic technique to reduce the risk of PIV catheter associated infections. A sterile probe cover, or sterile transparent membrane dressing and sterile gel must be included in those tools. Midline catheters are 3- to 8-inch-long catheters; are inserted into peripheral veins; and require the use of sterile probe covers for insertion. USGPIVCs are 2 or even 3 inches long. Why should there be a lower level of aseptic technique for one and not the other? The studies referenced in the INS Standards are descriptive studies using sterile technique for insertion of USGPIVC, which makes this Level V evidence. To my knowledge there are no higher-level studies comparing sterile vs non-sterile technique with USGPIV insertions. The literature search for these standards was completed in early 2015, and there may be newer studies published since then. Although the level of evidence is low at present, we know that PIVC associated infections do occur, yet they are not tracked and documented like CLABSI. Patients are often discharged before clinical signs and symptoms of infection are seen. PIVC associated infections are being seen in lawsuits now. I firmly believe that sterile technique is required for USGPIVC insertion. And all clinicians must focus on better aseptic techniques for insertion of all PIVCs!
Michael Jaqua
4/20/2017 09:05:37 am
I cannot believe there would be any pushback regarding the use of a sterile probe cover for placement of ultrasound-guided PIVs.
Gina Donato
4/28/2017 04:37:27 am
We just updated our PIVUS policy and were conflicted regarding sterile vs nonsterile gloves. With "no touch" technique after sterile prep do we need sterile gloves? Gina
Michael Jaqua
5/1/2017 03:13:46 am
Because infection prevention matters. 5/3/2017 10:05:19 am
Hi Gina, the INS Standards of Practice 2016 suggests that we consider using sterile technique for ALL PIVs, especially if you are changing them based on clinical indications and want to extend the dwell time. If using a long sterile probe cover, I would recommend sterile gloves. If using a large TSM dressing to cover the probe, your sterile gloves would be placed onto the non-sterile area of the probe. For regular PIVs, sterile technique is not supported by studies yet and we have very little data on infection risks from PIV. I know they happen from lawsuits I have seen. For USGPIV, usually you want that catheter to dwell for as long as possible and I would use sterile gloves. We definitely need much more data on these issues to refine the standards.
Lynn Hadaway
5/3/2017 10:09:39 am
Hi Gina, I would recommend using sterile gloves for USGPIV. However that could depend on whether you are using a long sterile probe cover or a large TSM dressing. A TSM dressing would not cover the entire probe and your gloved hands are touching the non sterile probe. The 2016 INS Standards of Practice recommends that sterile technique be considered for all PIVs. This is because many hospitals are not removing them based on clinical indications. The better the technique on insertion, the better chance of reaching the lengthy dwell time. I know of a hospital in NJ routinely using all sterile technique for USGPIV insertions and having great results. Comments are closed.
|
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|

 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861