 Nurses from many different practice areas frequently ask this question. The patient has many visible veins on their chest or breast area, so why can’t we use those for insertion of a short peripheral I.V. catheter when there are no veins in the upper extremity? Take a close look at the picture, especially how these veins appear.
There are many reasons why using these veins is not good practice. First, the nurse must be concerned about WHY those superficial veins of the chest are so visible. The answer here is simple – changes in venous return due to injury, surgery, or some type of disease process. There can easily be vein thrombosis or stenosis that is restricting the blood flow and causing these veins to be so prominent. Engorged veins of the chest are a classic sign of vein thrombosis. Infusion into these veins will add to the problem of venous return. The second thing to be concerned about is the tortuous nature of those veins. Notice in the picture below how these visible veins are not lying in a relatively straight path. It would be most difficult to get a catheter to advance into those veins. There is no method to distend these veins for venipuncture. The risk of infiltration/extravasation is a third factor. There are numerous cases of severe extravasation injury due to leakage from a CVAD insertion site and from a needle used for accessing an implanted port. I have seen lawsuits where a total mastectomy was required due to these events. Many times these questions come from nurses in the emergency department. And many times these nurses will need to give vesicant medications such as calcium chloride or calcium gluconate, 50% dextrose, or high concentrations of potassium – all are vesicants that can produce severe tissue damage if they leak from the vein into the subcutaneous tissue. Even if the prescribe I.V. therapy is only for fluids, the alteration in normal venous return will cause fluid to overflow the puncture site and into the subcutaneous tissue. The fourth factor is there is no research to support this practice and it is not recognized by any professional organization. Fortunately, there are much better alternatives. All nurses with responsibility for performing peripheral catheter insertion MUST have the skill of vein palpation. This skill can easily be learned. Practice palpating the upper extremity for veins before choosing a site on all patients. Always use the same finger of the same hand for this technique. Press downward and feel for an elastic rebound of a healthy vein beneath your fingertip. Do not simply rub your finger over the skin surface, as this will not provide useful information about the vein condition. If the vein feels hard or cord-like, it is sclerosed and should not be used. Palpation may not work for every patient due to vein changes from many courses of infusion therapy, or disease processes such as diabetes. Nevertheless, you may be surprised at the unseen, palpable veins you will be able to find when you have mastered this skill. If the situation requires rapid access, choose an intraosseous device. Again, insertion is a skill to be learned. The intraosseous route provides rapid assess and is now recommended when time is critical. Do not waste time searching for a peripheral vein and making many unsuccessful attempts. This delay only adds to the risk for the patient. Finally, if time is not a critical factor, use an infrared light device or ultrasound to locate veins in the upper extremity that you cannot palpate. Again, these are more skills that must be learned and your facility must make the investment into providing these devices. However, these devices are well documented to increase the success of peripheral venipuncture in patients with difficult venous access The bottom line is that superficial veins of the chest or breast area should never be used for insertion of a peripheral catheter because the risks are much greater than the benefits. Moreover, there are many other alternatives.
0 Comments
The growing discussion about the correct use of midline catheters brings up another related issue. What is the definition for vesicant and irritant? What are the differences and similarities? The following definitions are taken from the glossary of the 2011 Infusion Nursing Standards of Practice.
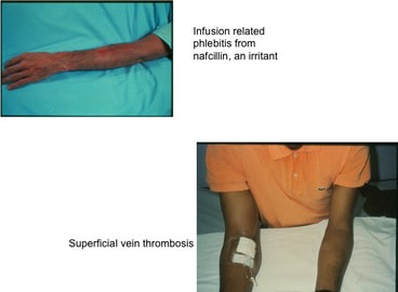 These definitions indicate a major difference of where the damage is taking place. For a vesicant, the damage is occurring in the subcutaneous tissue OUTSIDE of the vein. For irritants, the damage is occurring to the vein wall INSIDE the lumen. Vesicants cause tissue damage that may OR may not require surgical intervention. Notice in the definition the use of the word “or” – blistering, tissue sloughing OR necrosis. Blistering and tissue sloughing are tissue damage but necrosis may not be present. Time is required to heal the area, hopefully without any permanent tissue destruction. Necrosis requires surgical debridement and maybe even skin grafting to allow for complete healing. Vesicants produce this entire range of tissue injury with the damage occurring to the subcutaneous tissue at or near the point of where the fluid is escaping from the vein. This can be at the point of vein puncture or the catheter’s tip location or both. Irritants cause phlebitis (vein inflammation) and thrombophlebitis (thrombus plus inflammation), so the damage is occurring inside the vein lumen. This inflammatory process can produce severe edema but there is no infusing fluid leaking from the vein into the subcutaneous tissue. When peripheral catheters are used for infusion, this is occurring in superficial veins, thus the diagnosis of superficial thrombophlebitis. When it occurs with a PICC or other CVAD, it is most often a deep vein thrombophlebitis. The term, “extravasation” is referring to the leakage of vesicant fluid/medications into the subcutaneous tissue. But this term is not used when the event is from an irritant inside the vein lumen. Signs and symptoms often overlap between these 2 complications. It may be difficult for staff nurses to distinguish the difference and this is where the knowledge and skill of an infusion nurse is required. 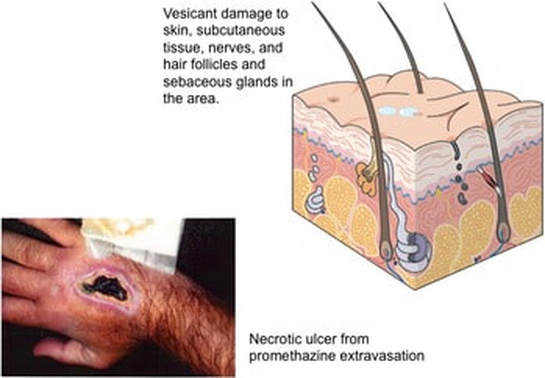 Have you checked out our new EBP Reports? These concise reports
 |
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861