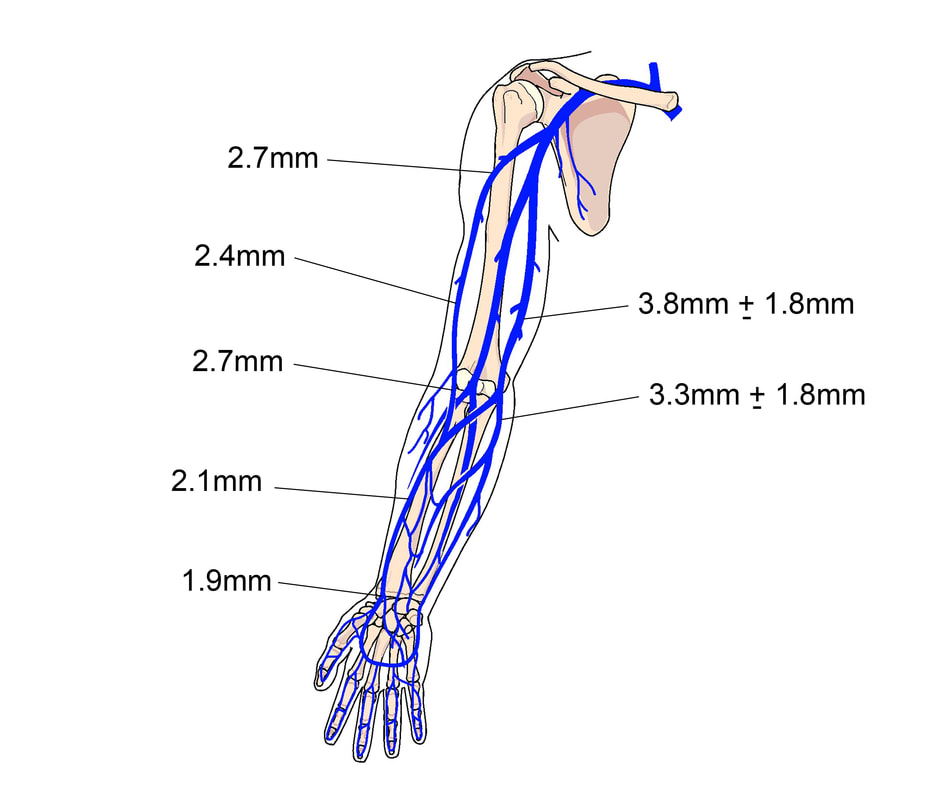
 Traditional methods to assess peripheral veins have relied exclusively on palpation of the vein lying under the skin. In many patients, t1he experienced inserter can easily locate veins that are not seen and determine their health by certain characteristics such as a hard, cordlike feeling. Palpation provides little information about the actual size of the vein and it is an educated guess about what size catheter the vein will accommodate. Until recently, there have been very few studies on the actual diameter of peripheral veins. An increasing awareness of the unacceptable outcomes associated with peripheral catheters1 is driving change. We now have several studies assessing the diameter of peripheral veins. An ultrasound study of peripheral vein anatomy reported that the average diameter of veins in the adult hand is 2 mm and the adult forearm is an average of 2.9 mm.2 Mapping superficial veins of the upper extremity is necessary for creation of arteriovenus fistulas and has provided useful information for the cephalic and basilic vein the entire length of the arm. 3 4 We also know from these and other studies that the cephalic vein does not always get larger in diameter as it moves up the arm and that the basilic vein is the largest diameter in only 55% of patients according to one study.5 Additionally, studies now point to contact between the catheter and vein wall as the source of endothelial damage leading to inflammation and thrombophlebitis. Pressure against the endothelial call layer causes release of von Willebrand Factor and Interleukin-8, both pro-inflammatory and pro-coagulant substances.6 Vascular visualization technology now allows a clear view of the vein and its pathway, venous valves and bifurcations. We can now improve these unacceptable outcomes by using visualization technology, plus incorporating all 3 types of peripheral catheters into our practice. Time to think about the lowly peripheral veins in a new way. References 1. Helm RE, Klausner JD, Klemperer JD, Flint LM, Huang E. Accepted but Unacceptable: Peripheral IV Catheter Failure. Journal of Infusion Nursing. 2015;38(3):189-203. 2. Gagne P, Sharma K. Relationship of Common Vascular Anatomy to Cannulated Catheters. International Journal of Vascular Medicine. 2017;2017. 3. Spivack DE, Kelly P, Gaughan JP, van Bemmelen PS. Mapping of Superficial Extremity Veins: Normal Diameters and Trends in a Vascular Patient-Population. Ultrasound in medicine & biology. 2012;38(2):190-194. 4. Ayez N, Van Houten V, De Smet A, et al. The basilic vein and the cephalic vein perform equally in upper arm arteriovenous fistulae. European Journal of Vascular and Endovascular Surgery. 2012;44(2):227-231. 5. Sharp R, Cummings M, Fielder A, Mikocka-Walus A, Grech C, Esterman A. The catheter to vein ratio and rates of symptomatic venous thromboembolism in patients with a peripherally inserted central catheter (PICC): a prospective cohort study. Int J Nurs Stud. 2015;52(3):677-685. 6. Weiss D, Avraham S, Guttlieb R, et al. Mechanical Compression Effects on the Secretion of vWF and IL-8 by Cultured Human Vein Endothelium. PloS one. 2017;12(1):e0169752. 
0 Comments
|
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861