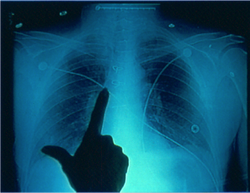
 The standard of care for all central vascular access devices (CVAD) is to know the anatomical tip location before infusion therapy is given through the catheter. A chest radiograph (CXR) to determine anatomical location of the catheter tip has long been the “gold standard” following placement of each CVAD. Nurses now insert the majority of PICCs, usually at the bedside or in a procedure room, as this is the most practical and cost effective process. Additionally the practice of nurse specialist is expanding to include insertion of other percutaneous centrally inserted catheters. Although many PICCs now use electrocardiograms (ECG) to determine tip location, there will always be patients in need of a CXR to confirm a CVAD/PICC tip location.
The nurse inserting the CVAD/PICC and assessing the CXR for tip position enhances the quality of care because timely results are known without delays in infusion therapy. This process also provides more documentation for appropriate information and management surrounding the insertion procedure. To enhance patient flow through the system and reduce costs of care, avoiding delays in treatment is paramount. Waiting on the radiologist or other physician for the “official” reading delays the delivery of critical fluids and medications. Requiring the nurse inserter to confirm tip location with a radiologist or other physician also delays infusion therapy. In many facilities, PICC insertion could be limited to the times when the radiologist is available. Or, the catheter is inserted, but cannot be used for infusion until a radiologist is available to assess the location and “release” it for use. Inadequate information about tip location from Radiology creates an unsafe situation for the patient. According to the Infusion Nursing Standards of Practice, nursing staff must know the specific anatomical location BEFORE infusion therapy is started (INS, 2006, S42-S43). Verbal information from Radiology can be vague and unacceptable such as, “Line is in good position” or “It is okay to use”. These statements do not convey the specific anatomic location and the written report may not be available for hours, even days. A nurse inserting CVAD/PICCs should have the knowledge of chest anatomy and physiology of blood flow. Also a nurse inserting a PICC can have the knowledge and skill to assess a CXR for correct catheter tip location. It is important to note that this is not the same as “reading a CXR.” The nurse-inserter is correlating the patient’s anatomy on the CXR to the CVAD/PICC tip location and position. Reading the CXR is medical practice for diagnostic purposes as it involves the complete assessment for all pathophysiological changes in the chest such as pneumonia or a pneumothorax or tumor. Confirmation of PICC tip location can now be done by assessing ECG. Competent nurses in many areas of clinical practice assess ECG rhythms to validate clinical assessment parameters and provide treatment based on that assessment. Likewise, an educated nurse with documented competency is qualified to assess the CVAD/PICC tip position by ECG or CXR assessment. The next question then becomes can the nurse-inserter provide instruction to the staff nurse that the CVAD/PICC is correctly positioned and can be used for infusion. In my opinion, if there is documented competency and well written and approved policy and procedures, then assessing a CXR and telling the staff nurse when it is acceptable for infusion is within the scope of practice for nurses who are inserting CVAD/PICCs. It is imperative to know the position of the board of nursing in the state where you practice about these issues. Most, but not all, state boards of nursing now use the scope of practice decision tree with questions for the nurse and employer to answer scope of practice questions. Principles of radiology, the process for assessing a CXR, and the legal issues of this practice are thoroughly discussed in our online course – Chest Radiograph Assessment and Central Vascular Access Devices. Learn more about assessing CXR from this online course, which includes a sample policy and procedure and competency assessment forms. By passing this online course, you also earn 4 CRNI recertification units! Comments are closed.
|
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861