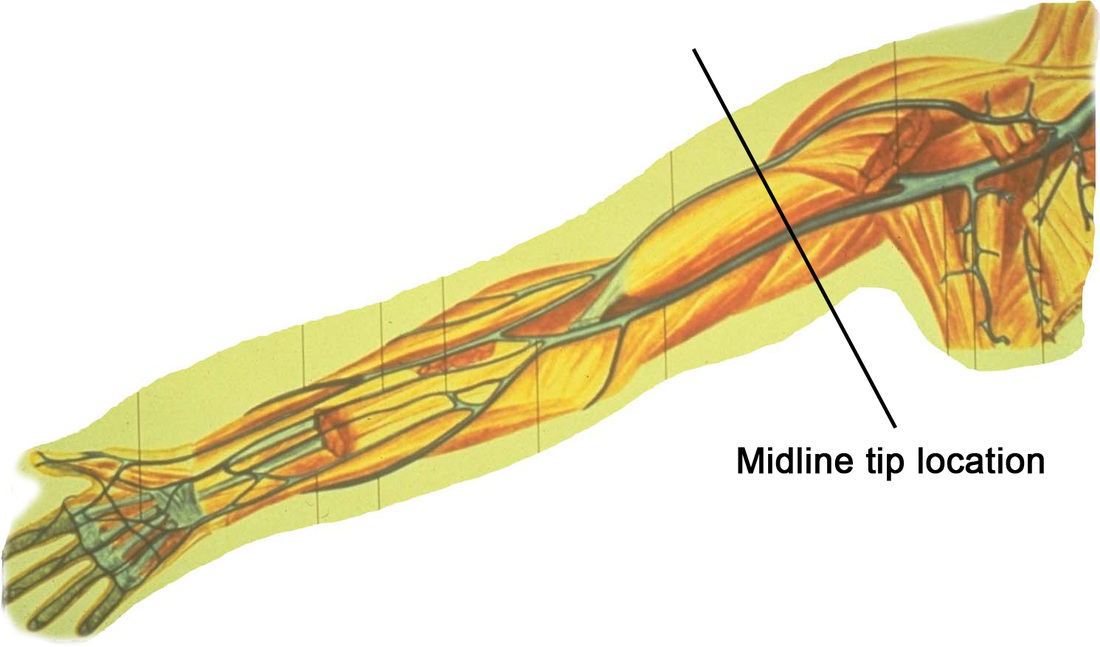
 There are currently several midline catheters available with a labeled indication for power injection of contrast agents. While the catheter are build to withstand the pressure that may be created with power injection, we need to ask another question – Is it safe to use a midline tip location for power injection of contrast agents? The simple answer is we don’t know yet.
The concern is the injection of a hypertonic contrast agent considered to be vesicants into the deep upper arm location of a midline catheter. Deep veins could mean that fluid in the tissue may go undetected and potentially damage large arteries and nerves in the area. Many clinicians report that a midline catheter will not typically produce a blood return, thus eliminating one component of a complete clinical assessment of catheter patency. One the positive side, evidence is showing that longer catheters are needed when ultrasound is used to access deep vessels. Higher rates of infiltration/extravasation are reported when deep veins are used, even with 1.8 and 2 inch long catheters. This may indicate tht a 3 inch long catheter could be safer than a 2 inch catheter in the veins of the upper extremity. At the present time, there is a distinct need for more research on midline catheters and the midline tip location. I am aware of 2 simple descriptive clinical studies on the newer midline catheters labeled for power injection. These studies included a brief statement about small numbers of patients having the midline catheter used for contrast injection. These studies did not include details of the types of contrast agents used, the rates of injection, or the dwell time of the midline catheter when the contrast was injected. Extravasation with contrast agents happens, although it is reported to have very low rates usually less than 1%. In my experience as an expert witness, I have seen about 15 cases of contrast extravasation however all have involved short peripheral catheters inserted in the hand, wrist or antecubital fossa. No cases have involved a midline catheter or midline tip location. The bottom line is we need more data for these critical clinical decisions.
Dudung
3/9/2016 04:48:56 am
The aim of midline application is in order to prevent iv insertion complication, compare to pheriperally catheter, as CDC guudeline..
Lynn Hadaway
3/9/2016 10:53:31 pm
Duding, midline catheters have complications just like all other VADs. Phlebitis, infiltration/extravasation, thrombosis, and infection happens with all types of catheters. Midline are no exception.
Pamela Jacobs
3/9/2016 09:50:40 pm
Thanks Lynn. My organization is in the middle of conducting a midline product evaluation and the manufacturers are selling the midline as power injectable although finding literature to support the use with injectors is near impossible. Our radiologists are reluctant or opposed to the use for the reasons you mentioned above. I agree, more research is needed to recommend or warn against using a midline for contrast. It is clear that the midline should not be used for vesicant chemotherapy. As midlines become more common place, the hope is so will more information about contrast, blood draws, use of fibrinolytic, etc. will be forth coming. Comments are closed.
|
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861