
The blood sample you just obtained from the central vascular access device looks more like a strawberry milkshake than a sample of human blood. In another situation, you could see small white floating pieces in the sample or when it settles, the plasma looks very cloudy. What is causing the different appearances? One problem is a lipemic blood samples; the cloudy, opaque or “strawberry milkshake” appearance is from fat in the bloodstream. Triglycerides greater than 1000 mg per dL (11.3 mmol per L) can easily cause this appearance. Or your patient may simply have eaten a large fatty meal a few hours before having the blood sample drawn. Another component of blood that creates a milky appearance is chylomicrons - a combination of fat globules and protein. This combination occurs in the small intestine, and moves through the intestinal walls into the lymph vessels. These vessels ascend to the upper thorax, merge into the thoracic duct which joins the left subclavian vein. The chylomicrons travel in the bloodstream until they are either stored or metabolized for energy. Given the close proximity of the thoracic duct and the CVAD tip location, it is easy to see why a blood sample drawn from a CVAD may be more likely to appear cloudy or milky. White blood cells and platelets may clump together to form a cellular aggregate. They may appear white or opaque and do not disperse when the container is rotated or shaken. Visible white particles composed of lipid or fat material may also appear in blood samples in patients with hypercholesterolemia. Studies of white particulate matter in stored blood have proven to be WBCs and platelets along with other cellular fragments. 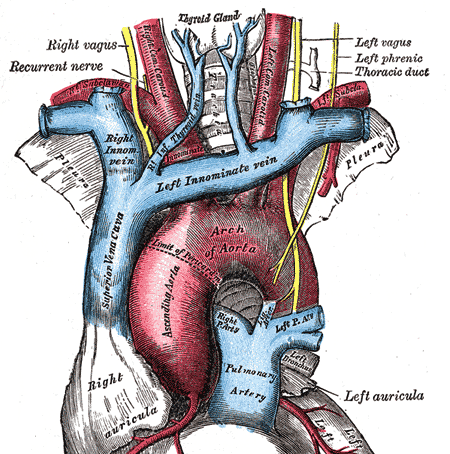
 Have you ever had a patient complain of strange heart flutters, palpitations, or even chest pain when a PICC is indwelling? What can be done and who should do it?
After PICC insertion, the tip is not stationary. Inserters make every attempt to get the catheter tip at the cavoatrial junction, however arm movement can and often does alter this location. For PICCs, this will usually means the tip moves inward, into the right atrium. This can cause the cardiac flutter feeling or your patient may complain of feeling a fast or irregular heartbeat. Retraction of the PICC by a very short distance may be needed to relieve these symptoms. Who should be doing this catheter repositioning – the nurse inserting the PICC or the primary care nurse? Legally speaking, this procedure may be within the legal scope of practice for both registered nurses, BUT a policy from your organization is necessary to direct who can actually perform this procedure. There are several decisions to be made before any central VAD is repositioned. Where was the original tip documented – precisely? How was this tip location confirmed – chest xray or ECG? According to the 2016 Infusion Therapy Standards of Practice, the tip of any CVAD can be anywhere from the lower third of the superior vena cava and extend into the right atrium by 2 cm. If the original placement was at the cavoatrial junction, arm movement may have taken the tip more than 2 cm into the right atrium and this indicates the need for retraction if the patient has any cardiac complaints. A chest xray may be necessary before this retraction to provide more precise information on the safe length that should be retracted. The adult superior vena cava is usually about 7 cm long. CVAD tips located in the mid to upper SVC are more prone to complications such as tip migration into the jugular vein and vein thrombosis. Retraction without a precise measurement could result in a suboptimal tip location which increases patient risk. The policy and procedure written and approved by each facility must address which nurse will be doing this procedure. It is my professional opinion that this catheter manipulation should only be performed by the nurse with documented competency with PICC insertion. It should not be performed by the primary care nurse, or anyone without the detailed knowledge and skills for PICC insertion. Retraction itself is not a difficult task, but there are many aspects of patient assessment, critical thinking and decision-making required. The facility policy should also require documented competency to perform this procedure, especially if the responsibility is given to the primary care nurse. Two standards of practice address this issue. Please read Standard 53 CVAD Malposition and don’t forget the Section Standards on page 103 as they apply to all standards in this section. The second standard is #5 Competency Assessment and Validation. You should also check with your state board of nursing for any specific statements they may have about PICC insertion and management.  The 2016 Infusion Therapy Standards of Practice used many “action” verbs to start the Practice Criteria statements. A quick look through this document shows “assess”, “use”, “perform”, “determine”, “choose”, “select”, and many others. But this examination of the document also reveals another word in common use – “consider”. Is there a difference in these verbs? If so, what is that difference?
This is an evidence-based document, meaning the committee searched the published literature and carefully evaluated all evidence. As indicated in the rating scale found on page S10 of the document, there is a hierarchy of these studies based on the study design. There are several ways to evaluate this found evidence. Multiple studies with good research design and study processes that produced consistent results received a high rating, usually a grade of I or II. These statements are the ones that begin with the strong action verbs. As you would imagine, this high level of evidence was not always found. Sometimes, the study design and process was good, but the outcome of several studies may be inconclusive or conflicting. This indicated the need for a lower rating. These practice criteria statements begin with “consider” and require a closer examination for your practice. These statements go on to provide specific criteria that should be contemplated. You may be using these statements to make decisions about a specific patient situation or to write facility policies and procedures. These “consider” statements will require more critical thinking on your part. You may need to think about all aspects of care for a specific patient or the needs of a larger patient population. The expertise or skill level of your staff, and the staffing mix such as RN versus LPN/LVN versus unlicensed assistants may need to be deliberated. Additionally, you may reach a different practice decision based on the venue of care, considering the differences between hospitals, skilled nursing facilities, an ambulatory clinic, or the home. The bottom line is that there continues to be many aspects of practice without concrete answers to every question. You may need to look up the references provided to obtain more details to guide your decision. This process requires a high level of critical thinking skills and good nursing judgment. The body of evidence is improving, however we will never have all the needed answers, so critical thinking is a necessary skill to develop. Pay attention to the action verbs and the rankings of evidence to reach the most appropriate decisions.  Catheter associated vein thrombosis can be a significant problem with some central vascular access devices, especially PICCs. The question about immediate removal is always first and foremost on the minds of most nurses. A color duplex ultrasound study can be used to show extensive thrombosis in either vein where the catheter lies. It may also demonstrate no blood flow in those same veins. Where should the removal procedure take place – in the patient’s room, a treatment room, or in Radiology under fluoroscopy? Who should do the removal procedure – primary care nurse, nurse inserting the PICC, primary physician, radiologists?
First, don’t be too quick to advocate for removal. Before you consider where and by whom the catheter will be removed, there are some other questions that should be addressed. Your answers to these questions may indicate that the catheter should be left in place. Does this patient continue to require a central venous catheter after considering the remaining length of infusion therapy and its characteristics? Is it possible that the infusion therapy is near the end and it may be discontinued or changed to another route? This will require reading the progress notes of the licensed independent practitioner(s) (LIP) and discussing the situation with them. Before you initiate this discussion, gather some additional information. If fluids are infusing, what is the patient’s ability to eat and drink? Are vital signs normal and stable? What medications are being given? What is the anticipated length of time remaining on this plan of care? If only a few more days, a change to oral medication may be possible. Next assess where the catheter is located and how well it is functioning. Is the catheter tip in the recommended position in the lower SVC near or at the cavoatrial junction? Is the catheter functioning with a good blood return and no resistance to fluid flow through the catheter? If the catheter is correctly positioned and there is a blood return and there is no resistance to flushing or fluid infusion, this strongly favors leaving the catheter in place. Next consider all systemic signs and symptoms the patient may have. Are there any signs or symptoms, concern or thoughts of bloodstream infection being present? If yes, this could mean an infected thrombus and will usually mean catheter removal. Is the patient complaining of pain or any type of excessive discomfort in the arm, neck, shoulder, or chest, especially on the ipsilateral side of the catheter? These complaints may mean it is more than the patient is able to tolerate, however treatment may help to improve those complaints. Immediate removal when there is a need for another CVAD insertion may not be the best option. The next catheter could easily produce a similar event on the other side, so the goal is usually to leave it in place. The patient should be treated for DVT with systemic anticoagulation for as long as the CVAD is needed and for 3 months after it is removed. Information about this is found in two INS Standards - Standard 52 CVAD Associated Thrombosis and Standard 44 VAD Removal. The medical references are two evidence based guidelines. You might want to find these and share with colleagues and appropriate committees in your facility. Both of these publications can be downloaded free of charge. Click below to get the full text. Kearon, C., Akl, E. A., Comerota, A. J., Prandoni, P., Bounameaux, H., Goldhaber, S. Z., . . . Dentali, F. (2012). Antithrombotic therapy for VTE disease: antithrombotic therapy and prevention of thrombosis: American College of Chest Physicians evidence-based clinical practice guidelines. CHEST Journal, 141(2_suppl), e419S-e494S. http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3278049/pdf/112301.pdf Debourdeau, P., Farge, D., Beckers, M., Baglin, C., Bauersachs, R. M., Brenner, B., . . . Bounameaux, H. (2013). International clinical practice guidelines for the treatment and prophylaxis of thrombosis associated with central venous catheters in patients with cancer. J Thromb Haemost, 11(1), 71-80. doi:10.1111/jth.12071 http://onlinelibrary.wiley.com/doi/10.1111/jth.12071/epdf  Nurses and most of the general public know that Florence Nightingale is known as the Lady with the Lamp. But did you realize that she could also be called the Lady with the Pie Chart? She was known for her mathematical genius and use of statistics. She transformed those numbers from boring, meaningless tables to colorful diagrams and was able to demonstrate that more British soldiers were dying from disease than battlefield wounds. Click here to see some of her work.
While we celebrate her work and her birthday on May 12, we can still learn from her example. Notice that she is collecting and using her own internal data. She did not use data from the American Revolution or the War of 1812, but data from the hospital in Scutari during the Crimean War. Can you just image the backlash from those British army generals if she has used data from other wars? I can hear comments like a different war, a different climate, different continent, different types of guns, etc. Translate this to your current situation and it is really not that much different. Data from your facility on infusion-related outcomes such as complication rates, productivity and workload, and medication errors will be stronger than data from outside. Data from published studies are beneficial for benchmarking – are we better or worse than what is published? You will not know the answer unless you collect and analyze your own statistics. Internal data is about your patient population, skills and issues with your staff, and deficits or achievements in your own processes. Unlike Miss Nightingale, we now have computers, Excel and PowerPoint to enliven our data. Just imagine what she could have accomplished with our present data tools. The sky is the limit for what we can achieve as nurses inserting and managing vascular access devices and delivering infusion therapies! Happy Birthday, Miss Nightingale and thanks for your legacy!  Within the past few years, advertising for many new types of midline catheters state the dwell time of up to 29 days. Does this mean that the catheter should be removed on or before the 29th day? The answer is a definite NO.
The 2016 Infusion Therapy Standards of Practice states, “VADs are not removed based solely on length of dwell time because there is no known optimum dwell time.” Then what is the basis for this statement about midline dwell time of 29 days? That answer comes from a guidance document released by the FDA in 1995. This document included a list of information that must be included in the manufacturer’s original submission to the FDA to obtain clearance to sell the device in the United States. The manufacturer must classify the device into one of two groups – “Class II for short-term intravascular catheters (less than 30 days), Unclassified for long-term (more than 30 days) percutaneous intravascular catheters”. This classification is made long before there is any clinical use of the device, therefore clinical outcomes are not known when this submission is made. Reasons for removal of all VADs should be based on clinical findings. What does the insertion site look like? Are there any complaints from the patient about the device? Is it still functioning without resistance to flushing and producing a blood return that is the color and consistency of whole blood? Is the catheter still needed for the patient’s plan of care? These are the factors to consider about removal of any VAD including midline catheters. So forget the clock or calendar to determine when the catheter should be removed. Learn more about Midline Catheters in our newly updated course, Midline Catheters: What, Why, When.  The instructions have recently changed. Now the package insert for all I.V. fat emulsion (e.g., Intralipid, Nutrilipid) states to use a 1.2-micron filter for all infusion. Previous instructions were not as specific, stating that filters were not recommended or that a filter of less than 1.2-micron pore size was not to be used.
This brings up several questions about the most appropriate filtration for infusing all parenteral nutrition solutions. When all components are admixed together in one solution container (ie, 3-in-1 or Total Nutrient Admixture), the recommendation has always been to use an in-line 1.2-micron filter for infusion. IVFE will not pass through filters with a smaller pore size. The concern was and still is cracking the fat emulsion, possibly resulting in a fat embolism. What about filtration for a 2-in-1 solution containing protein, carbohydrates, and other additives? The practice has been to use a 0.2-micron filter on this solution to ensure removal of all particulate matter and microorganisms. IVFE was piggybacked below the filter or given through a separate catheter with no filtration. Now the IVFE requires a 1.2-micron filter regardless of where it is infused. There are several options for configuring the filters. According to 2016 INS Standards of Practice and a 2014 ASPEN guidelines document, a 0.22-micron filter is needed for the 2-in-1 PN solution due to particulates from the compounding process and microorganisms that could enter the system. To follow these new IVFE manufacturer instructions, 2 filters of 2 different sizes must be used - a 1.2-micron filter on the IVFE and a 0.22 micron filter on the 2-in-1 PN. The other option would be to use a 1.2-micron filter in the system and infuse both 2-in-1 PN and IVFE thru the same filter. This could be considered the same as infusing a 3-in-1 PN solution thru a 1.2-micron filter. To make the clinical decision about filters, I would want to know what filtration, if any, was done by the pharmacy during the compounding process. If pharmacy is filtering, what pore size filter is being used? To reduce microbial contamination, I would strictly enforce the policy of NOTHING being injected or piggybacked into this system and the system would ONLY be taken apart when it is time to change the entire administration system once every 24 hours. 
The number of venipuncture attempts to insert a short peripheral catheter is a critical factor in the ultimate health of your patient’s veins. The 2016 Infusion Therapy Standards of Practice call for no more than 2 attempts per clinician with a limit on the total number of attempts to 4. After 4 unsuccessful attempts, it is time for a careful assessment of VAD needs and discussion with the patient’s providers to decide on the most appropriate options. Many experts would argue that 4 attempts are too many! Think about those 4 veins that have been punctured, damaged and will now have a small amount of scar tissue.
We have all encountered those patients with difficult venous access – no peripheral veins can be seen or palpated. Or the veins that can be felt are hard and rope-like meaning they are sclerosed. I have often wondered how many failed venipuncture attempts these patients have endured. Many healthcare issues cause damage to the vein wall – some within the patient’s control such as smoking and some due to chronic illnesses such as diabetes. The number of patients with chronic diseases requiring frequent venipuncture is growing. Blood sampling, receiving diagnostic tests such as CT scans with I.V. contrast, or courses of antibiotics for frequent infections translates to numerous venipunctures. But failed venipuncture attempts are directly related to the skill and judgment of the clinician. Vein damage occurs regardless of whether the attempt was successful or not. The goal is vein preservation so that peripheral veins remain available for the entire lifetime. Many times, a central venous access device is needed for no other reason than an absence of peripheral veins. A CVAD carries the greatest risk of bloodstream infection and vein thrombosis, so the goal is to use them ONLY when the length, frequency, and characteristics of the infusion therapy demand the tip location in the superior vena cava. By protecting patient’s peripheral veins, these goals are possible. Never make a venipuncture attempt blindly, without being able to see or feel a vein in good condition. Assess both extremities for the total number of sites available. If there are very few sites, and you do not think your venipuncture skill is sufficient for the level of difficulty, call the infusion/VA nurse or another clinician with more experience and inform them that near-infrared light or ultrasound may be needed. Consider the length of therapy and the characteristics of the prescribed medications. Don’t stick a vein in a finger or some other odd location just for the sake of saying you can do it. And finally work to change those terrible policies requiring that the patient’s nurse make a certain number of attempts before they call for assistance. These policies add to the problem of vein wasting and ignores the goal of peripheral vein preservation.  This issue continuous to cause much confusion among nurses and others using any type of vascular access device (VAD). You were probably told that ONLY a 10 mL syringe or a syringe with a barrel the same size as a 10 mL syringe could be attached to any VAD. So you have been transferring small volume medications to a larger syringe to follow this rule. Now it is time to learn the facts so you can base your practice on evidence. It is true that a larger syringe size (ie. 10 mL) will generate less pressure on injection than a smaller syringe (ie, 3 mL or 5 mL). That was the basis for the outdated “rule” about only using a 10 mL syringe. But the issue is actually catheter damage and syringe size is only one factor, and I would hasten to add, not the most important factor! Catheter damage depends on 2 things happening.
Two important documents now address this issue. The 2016 Infusion Therapy Standards of Practice states that the functionality of all VADs should first be assessed with a saline-filled 10 mL syringe. Patency is confirmed when there is NO resistance, a blood return that is the color and consistency of whole blood, and the absence of any signs or symptoms of VAD complications. Pay attention to any complaints the patient may have. Strange sensations in the chest, neck, shoulder or extremity are not normal and require further investigation. If the VAD is patent, proceed with giving the medication in a syringe that is appropriate for the dose of medication being given. Yes, that means using a 3 mL syringe. The Infusion Therapy Standards can be purchased here. The second document is from the Institute for Safe Medication Practices, Safe Practice Guidelines for Adults IV Push Medications. This document contains lots of great information about avoiding unnecessary drug dilution. It strongly states to NOT use a prefilled flush syringe to dilute medications, providing the reasons for this. There is also similar guidance on assessing VAD patency with a 10 mL diameter-sized syringe and to use a syringe appropriately sized for the medication, pointing out the risk associated with a syringe-to-syringe transfer of the drug. This document is a free download. Many new documents are now available to guide your clinical practice, including those we discussed in this week’s blog message above. You may have many questions about these or other new guidelines documents. Lynn Hadaway has been an author on many of these documents and can help you to understand their content. We are setting aside time each month for discussing your questions. Register for our monthly video conference session on Thursday, April 14 at 12 noon ET. Submit your questions before the scheduled day. Join the conference with Lynn Hadaway to get more information, explanation, and clarification on your questions. 
 Yes, this is indeed a practice to consider, however when and how it is done requires some practice changes. The 2016 INS Standard on Phlebotomy states to consider using a peripheral catheter for blood sampling in pediatric patients, adults with difficult venous access, the presence of bleeding disorders and the need for serial tests. The issue is the point in the procedure when the sample should be obtained. The answer is after the procedure is completed.
Tourniquet time is the reason for this recommendation. The length of time that a tourniquet should be on for drawing all blood samples is no more than 1 minute. Lengthy tourniquet times cause changes in the venous endothelial that produces changes in the lab values for many tests. Longer tourniquet time is usually needed for insertion of a short peripheral catheter using customary techniques of seeing and feeling the vein. Instead of drawing the sample as you insert the catheter, finish the procedure with complete securement and dressing. Then draw the sample. This allows for the tourniquet to be removed and the normal blood flow to flush away the blood containing the cellular substances that leads to alterations in lab values. Learn more about the decisions for obtaining a blood sample in our online course – Blood Sampling: Venipuncture or VAD? The focus is now on preventing hospital-acquired anemia associated with blood sampling and several other issues. |
Author: Lynn HadawayLynn Hadaway is an international thought leader in infusion therapy and vascular access, having been in this practice for more than 40 years. Her experience comes from hospital-based infusion teams, device manufacturers, and continuing education services. Her journal and textbook publications are extensive. She also maintains board certification in infusion nursing (CRNI) and nursing professional development (RN-BC). 
Categories
Archives
May 2019
|
 RSS Feed
RSS Feed
Copyright © 2020 Lynn Hadaway Associates, Inc. | P.O. Box 10, Milner, GA 30257 | 770-358-7861